
|
|
|
|
|
||
|
|
||
| SUBMIT IDEA OR EXPERIENCE | CONFERENCE/WORKSHOP CALENDAR |
An Overview of Multiple Sclerosis - By Jameson HeisePathophysiology/Diagnosis Multiple Sclerosis is an inflammatory demyelinating disease of the central nervous system. This disease is a "disorder of the brain and spinal cord in which degeneration of the myelin sheath that surrounds the axon occurs, leading to an interruption of nerve impulses" (Stopka, 1997, pp.131). The cause of the disease is unknown but one theory under intense research is that it is an autoimmune disease, mediated by active T cells that break through the blood-brain barrier and degrade myelin (Petajan & White, 1999). Relapsing-remitting multiple sclerosis, the type present in 80 percent of patients, is usually seen in the second or third decade of life with a female to male ratio of 2:1 (Noseworthy, Lucchinetti, Rodriguez, & Weinshenker, 2000). "Most patients have signs and symptoms for about 15 to 25 years and may stabilize" (Stopka, 1997, pp. 131). The other twenty percent have primary progressive multiple sclerosis, which is a gradual degeneration of the central nervous system. The way the disease progresses is highly unpredictable regarding individual patients (Noseworthy, et al., 2000). Relapsing-remitting multiple sclerosis has many signs and symptoms associated with its onset: sensory disturbances, unilateral optic neuritis, diplopia (double vision) Lhermitte’s sign (trunk and limb paresthesias evoked by neck flexion, limb weakness, clumsiness, gait ataxia (walking coordination), and neurogenic bladder and bowel symptoms (Noseworthy, et al, 2000). These symptoms are typically seen in the beginning stages of relapsing-remitting multiple sclerosis and are associated with some loss of central nervous system function. Further progression of the disease will lead to cognitive impairment, depression, emotional lability (instability), dysarthria (difficulty in articulating words), dysphagia (difficulty swallowing), vertigo, progressive quadriparesis, sensory loss, ataxia tremors, pain, sexual dysfunction, spasticity, and other problems of the central nervous system may result (Noseworthy, et al, 2000). The progression of the disease is usually associatied with an increase in the severity of dysfunction in the central nervous system. Relapsing-remitting multiple sclerosis has periods of worsening followed by periods of milder symptoms. Table 1 (Cohen, Kinkel, Ransohoff, Rudick, Weinstock-Guttman, 1997)
Effects of MS The negative symptoms associated with MS create a hurdle for MS patients
in their daily life and physical activities. MS causes discomfort, decreased
coordination, and decreasing strength. Decreases in ability to function
properly may prevent some people from performing activities that were
once ordinary. This reduction in physical activity may have direct implications
on the patient's quality of life and future health. Drug Therapy Corticosteroids are the chief treatment for acute relapses of MS. Treating patients with corticosteroids may help restore the blood-brain barrier, reduce edema, and improve axonal conduction. Corticosteroids are able to shorten the time spent in relapse and accelerate the recovery phase. Methylprednisolone quickly works to recover from relapse with consistent benefits and minimal side effects (Cohen, et al, 1997). Interferon beta is another form of treatment usually for less severe cases of MS. There are two types of interferon beta, 1a and 1b, both approved by the FDA. Tests on interferon beta 1b have proven to reduce disability and disease activity. Interferon beta 1a, according to recent research, increased the length of time to the progression of disability by about six months. Another significant finding was that it lowered the probability and severity of disability (Cohen, et al, 1997). Glatiramer acetate is a synthesized chemical that mimics the myelin basic protein. With glatiramer acetate annual relapse rates are approximately 29 percent lower and the proportion of patients without a repeated relapse was higher. This form of drug therapy provides an alternative to interferon beta treatment and was approved by the FDA in 1997 (Cohen, et al, 1997). Azathioprine is another treatment for MS which reduces the rate of relapse. The drug has no effect on the progression of disability, but is an alternative to other drugs (Cohen, et al, 1997). This drug would only be a good choice if the patient responded to none of the other drugs with more benefits. In progressive multiple sclerosis, methotrexate is taken orally in low doses. This treatment may work by inhibiting cell-mediated and humoral immunity or the anti-inflammatory effects. The main benefit seen is less disease progression (Cohen, et al, 1997) which directly impacts the patient's quality of life. Other immunosuppressive drugs have been used but the benefits are minimal and usually accompanied by negative side effects. Table 1 (Noseworthy et al)
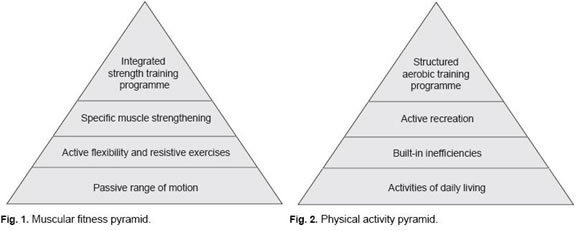
"Multiple sclerosis symptoms may lead to physical inactivity associated with the development of secondary diseases. People with multiple sclerosis are thus challenged by their disability when attempting to pursue an active lifestyle compatible with health-related fitness" (Dressendorfer & White, 2004, pp. 1077-1078). While many effects of MS may be debilitating, the benefits associated with good therapy and exercise are crucial. Combining physical activity with the drug therapy will give the patient with MS the greatest opportunity to stay healthy. Some of the medical community is still unsure of the effects of exercise on MS patients, "however, a growing number of studies indicate that exercise in patients with mild-to-moderate MS provides similar fitness and psychological benefits as it does in healthy controls" (Dressendorfer & White, 2004, pp. 1078). The patient must have an assessment by the proper physician regarding specific physical abilities and limitations. A patient's current level of fitness may be difficult to judge because of fluctuations in fatigue, lack of coordination, weakness, and ataxia. Some patients with MS have varying abilities in their extremities which allow for varied levels of activity (Petajan & White, 1999). The article Recommendations for Physical Activity in Patients with Multiple Sclerosis by Petajan and White provided a useful diagram for muscular fitness and physical activity.
Designing a program that incorporates these aspects of exercise will create a well rounded approach specific to the needs of the patient with MS. These fitness pyramids focus on overall health and quality of life including strength, flexibility, aerobics, recreation, and daily living. Working with a patient on balance or any fitness component will have a direct impact on a debilitative symptom of their disease. Keeping exercise and activities fun and specific to a patient will improve the patients overall physical fitness, ability to function on a daily basis, and develop a desire to remain in a fitness program. Adapted Therapy Adapted physical therapy has great uses when working with patients that may have some limitations. When trying to work on balance you may play a game where the patient is on an unstable surface (gym mat or trampoline) and you throw a ball back and forth. Cardiorespiratory training techniques may include stationary cycling (arms and/or legs), swimming, and treadmill. Exercise bouts should be coupled with alternating rest periods because of decreased endurance capacity (Dressendorfer & White, 2004). Resistance training in a pool with floating equipment allows for an environment that is easier to balance and support body weight. Resistance using machine weights, resistance bands, and other equipment is suitable also. If the patient is having trouble walking unassisted then the pool offers the opportunity to walk while bearing less weight. Playing any number of sports with your patient allows for skill development and strength gains. Many sports need little adaptation to include people with limitations. Opening up a sport to an individual with a disability allows them to play in a more inclusive social environment. Some examples of sport modification include: Basketball – lowering the rim, providing wheelchairs, an alternative basket, multiple balls for maximum participation Soccer – providing wheelchairs, a larger ball, play with sticks, multiple balls Volleyball – lowered net, lighter/bigger ball, more people, multiple balls The amount of adaptation you apply to activities to suit your patient is only limited by creativity. Countless adaptations can be made to accommodate almost any type of disability. Conclusion Multiple sclerosis is a serious disease that must be worked with to
avoid disability. Working through physical and drug therapies can greatly
increase the quality of life in many patients with MS. Dressendorfer, R. H., & White, L. J. (2004). Exercise and Multiple
Sclerosis. Sports Medicine, 34(15), 1077-1100. Noseworthy, J. H., Lucchinetti, C., Rodriguez, M., & Weinshenker, B. G. (2000). Multiple Sclerosis. The New England Journal of Medicine, 343(13), 938-952. Petajan, J. H., & White, A. T. (1999). Recommendations for Physical Activity in Patients with Multiple Sclerosis. Sports Medicine, 27(3), 179-191. Stopka, C. (1997). An Overview of Common Disabilities Which Often
Worsen With Age But Can Improve With Exercise. Applied Special Physical
Education & Exercise Therapy (3rd ed., pp. 131-132). Burgess Publishing.
Copyright © 1999-2007 | PELINKS4U All Rights Reserved |
|
|